CARDIOLOGY

HEART SOUNDS
Split S2 (pulmonary valve closes much later): PS, Pulmonary HTN, RBBB, PE
Fixed Split: ASD, VSD, MR
Paradoxical split (aortic valve closes much later): AS, HTN, LBBB
S3 (increase flow): Chronic MR, CHF, PDA, benign in kids and pregnancy
S4 (decrease compliance) : aortic MR, HOCM, LVH, AS, ischemia
PULSES
Tardus: AS
Bisferiens: HCM
Alternans: severe CHF
Paradoxus: cardiac tamponade, SVC Obstruction
Tardus: AS
Bisferiens: HCM
Alternans: severe CHF
Paradoxus: cardiac tamponade, SVC Obstruction
MURMURS http://www.easyauscultation.com/heart-sounds?gclid=CJ2vyK2B6b8CFYhcMgodeQYASQ
*SYSTOLIC
- Holosystolic: MR, TR, VSD
- Mid systolic murmur: AS, PS
- Late systolic murmur: MVP
* DIASTOLIC
- Mid diastolic: MS, TS, ASD
- Late diastolic: Atrial myxoma
- Early: AR, PR
*SYSTOLIC
- Holosystolic: MR, TR, VSD
- Mid systolic murmur: AS, PS
- Late systolic murmur: MVP
* DIASTOLIC
- Mid diastolic: MS, TS, ASD
- Late diastolic: Atrial myxoma
- Early: AR, PR
KUSSMAUL SIGN
Neck vein distension on inspiration
Seen in constrictive pericarditis, Cardiac tamponade and Rt ventricular infarction.
Neck vein distension on inspiration
Seen in constrictive pericarditis, Cardiac tamponade and Rt ventricular infarction.

HYPERTROPHIC CARDIOMYOPATHY (HOCM)
S4
Pulse bisferiens
Murmur increased by standing and valsalva
Murmur decreased by handgrip, squatting, sitting
Amyl nitrate (decreases afterload) increases HOCM, MVP and AS
Post PVC (decreases afterload) increases HOCM & AS, decrease MVP
S4
Pulse bisferiens
Murmur increased by standing and valsalva
Murmur decreased by handgrip, squatting, sitting
Amyl nitrate (decreases afterload) increases HOCM, MVP and AS
Post PVC (decreases afterload) increases HOCM & AS, decrease MVP

ATRIAL SEPTAL DEFECT
Ostium secundum atrial septal defect, located in the midportion of the atrial septum,(75% of cases ) . Usually isolated congenital cardiac abnormality. Right-sided chamber dilatation ( left-to-right shunt)
Ostium primum atrial septal defect is located in the lowest portion of the atrial septum. Usually associated with a cleft in the anterior mitral or tricuspid valve leaflets (leading to valve regurgitation) and with a ventricular septal defect or aneurysm of the membranous ventricular septum.
Inferior vena caval and unroofed coronary sinus atrial septal defects are both very rare.
PHYSICAL EXAM: Fixed splitting of the S2 and a right ventricular heave. A pulmonary midsystolic flow murmur and a tricuspid diastolic flow rumble caused by increased flow through the right-sided valves from a large left-to-right shunt may be heard.
The jugular venous pressure may be normal, or a and v waves may be equal.
DIAGNOSIS
TTE
EKG:
- In ostium secundum atrial septal defect : right axis deviation and incomplete right bundle branch block.
- In ostium primum atrial septal defect: first-degree atrioventricular block, left axis deviation, and right bundle branch block. Left atrial enlargement may result from mitral valve regurgitation from the cleft.
CXR: RA and RV enlargement, a prominent pulmonary artery, and increased pulmonary markings in both lung fields.
TREATMENT
- Small atrial septal defects (<5 mm) with no evidence of RV volume overload may not require closure unless associated with paradoxical embolism.
- Atrial septal defects with evidence of RV volume overload on echocardiography usually only cause symptoms after the second or third decade of life. Closure is indicated to reduce or prevent long-term complications such as atrial arrhythmias, exercise intolerance, paradoxical embolism, right-sided heart failure, and irreversible pulmonary hypertension. Even in adults, closure of large defects improves survival and relieves symptoms.
**The rate of late atrial fibrillation after ASD closure increases with age at the time of intervention; > 50% older than 40 years when closure is performed develop late atrial arrhythmias.
Ostium secundum atrial septal defect, located in the midportion of the atrial septum,(75% of cases ) . Usually isolated congenital cardiac abnormality. Right-sided chamber dilatation ( left-to-right shunt)
Ostium primum atrial septal defect is located in the lowest portion of the atrial septum. Usually associated with a cleft in the anterior mitral or tricuspid valve leaflets (leading to valve regurgitation) and with a ventricular septal defect or aneurysm of the membranous ventricular septum.
Inferior vena caval and unroofed coronary sinus atrial septal defects are both very rare.
PHYSICAL EXAM: Fixed splitting of the S2 and a right ventricular heave. A pulmonary midsystolic flow murmur and a tricuspid diastolic flow rumble caused by increased flow through the right-sided valves from a large left-to-right shunt may be heard.
The jugular venous pressure may be normal, or a and v waves may be equal.
DIAGNOSIS
TTE
EKG:
- In ostium secundum atrial septal defect : right axis deviation and incomplete right bundle branch block.
- In ostium primum atrial septal defect: first-degree atrioventricular block, left axis deviation, and right bundle branch block. Left atrial enlargement may result from mitral valve regurgitation from the cleft.
CXR: RA and RV enlargement, a prominent pulmonary artery, and increased pulmonary markings in both lung fields.
TREATMENT
- Small atrial septal defects (<5 mm) with no evidence of RV volume overload may not require closure unless associated with paradoxical embolism.
- Atrial septal defects with evidence of RV volume overload on echocardiography usually only cause symptoms after the second or third decade of life. Closure is indicated to reduce or prevent long-term complications such as atrial arrhythmias, exercise intolerance, paradoxical embolism, right-sided heart failure, and irreversible pulmonary hypertension. Even in adults, closure of large defects improves survival and relieves symptoms.
**The rate of late atrial fibrillation after ASD closure increases with age at the time of intervention; > 50% older than 40 years when closure is performed develop late atrial arrhythmias.

|

|

In ostium secundum atrial septal defect : right axis deviation and incomplete right bundle branch block.
|

In ostium primum atrial septal defect: first-degree atrioventricular block, left axis deviation, and right bundle branch block. Left atrial enlargement may result from mitral valve regurgitation from the cleft.
|

AORTIC ANEURYSM indications for surgery
* Thoracic aneurysm >6cm or expanding, putting pressure to other structures or if traumatic in origin
*Abdominal aneurysm > 5cm or expanding
* Thoracic aneurysm >6cm or expanding, putting pressure to other structures or if traumatic in origin
*Abdominal aneurysm > 5cm or expanding
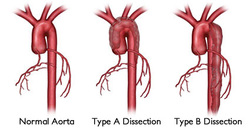
AORTIC DISSECTION (intimal tear).
Associated with bicuspid aortic valve (ascending aorta).
Major cause of death in Marfan syndrome.
Types
*Ascending or Type A or DeBakey I&II
*Descending or Type B
DX: CT OR MRI. TEE for descending aortic dissection
Tx: Decrease BP with B blockers and nitroprusside
Ascending dissections are at greater risk for rupture, so ALWAYS do surgery. Descending dissection treated medically.
Associated with bicuspid aortic valve (ascending aorta).
Major cause of death in Marfan syndrome.
Types
*Ascending or Type A or DeBakey I&II
*Descending or Type B
DX: CT OR MRI. TEE for descending aortic dissection
Tx: Decrease BP with B blockers and nitroprusside
Ascending dissections are at greater risk for rupture, so ALWAYS do surgery. Descending dissection treated medically.

ENDOCARDITIS
Suspected if an abnormal murmur is heard on examination, particularly if fever.
Etiology: Most cases of native valve endocarditis : streptococcal and staphylococcal species. Less common pathogens causing culture-negative or slow-growing endocarditis include HACEK organisms (Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, and Kingella), fungi, and mycobacteria.
Dx: Transthoracic echocardiography (sensitivity of 50% to 80% for detecting vegetations).
Transesophageal echocardiography ( sensitivity and specificity 95%). Test of choice to identify a paravalvular abscess.
Criterias for Endocarditis: Definite Endocarditis 2 major criteria or 1 major and 3 minor criteria or 5 minor criteria
* Major Criteria : Persistently positive blood cultures of organisms typical for endocarditis. New valvular regurgitation. Positive echocardiogram.
* Minor Criteria: Predisposing condition or drug use. Fever. Embolic vascular phenomena. Immunologic phenomena (eg, glomerulonephritis, rheumatoid factor) Positive blood cultures not meeting major criteria
Prophylaxis:
* Prosthetic cardiac valve
* Previous infective endocarditis
* Congenital Heart Disease: unrepaired cyanotic CHD or completely repaired with prosthetic device
* Cardiac transplantation recipient who develop valvular disease
Suspected if an abnormal murmur is heard on examination, particularly if fever.
Etiology: Most cases of native valve endocarditis : streptococcal and staphylococcal species. Less common pathogens causing culture-negative or slow-growing endocarditis include HACEK organisms (Haemophilus, Actinobacillus, Cardiobacterium, Eikenella, and Kingella), fungi, and mycobacteria.
Dx: Transthoracic echocardiography (sensitivity of 50% to 80% for detecting vegetations).
Transesophageal echocardiography ( sensitivity and specificity 95%). Test of choice to identify a paravalvular abscess.
Criterias for Endocarditis: Definite Endocarditis 2 major criteria or 1 major and 3 minor criteria or 5 minor criteria
* Major Criteria : Persistently positive blood cultures of organisms typical for endocarditis. New valvular regurgitation. Positive echocardiogram.
* Minor Criteria: Predisposing condition or drug use. Fever. Embolic vascular phenomena. Immunologic phenomena (eg, glomerulonephritis, rheumatoid factor) Positive blood cultures not meeting major criteria
Prophylaxis:
* Prosthetic cardiac valve
* Previous infective endocarditis
* Congenital Heart Disease: unrepaired cyanotic CHD or completely repaired with prosthetic device
* Cardiac transplantation recipient who develop valvular disease

Roth Spots

|


|

RBBB
Criteria:
* QRS >120 ms (3 boxes)
* rsr′, rsR′, or rSR′ in leads V1 or V2. .
* S wave of greater duration than R wave or greater than 40 ms in leads I and V6 in adults.
Criteria:
* QRS >120 ms (3 boxes)
* rsr′, rsR′, or rSR′ in leads V1 or V2. .
* S wave of greater duration than R wave or greater than 40 ms in leads I and V6 in adults.

LBBB
Criterias
* QRS >120 ms
* Monophasic R wave in I and v6
* rS or Q in lead V1
Criterias
* QRS >120 ms
* Monophasic R wave in I and v6
* rS or Q in lead V1
AFIB ANTICOAGULATION
